MindMap Gallery French Revolution: Causes, Phases, and Legacy
French Revolution: Causes, Phases, and Legacy
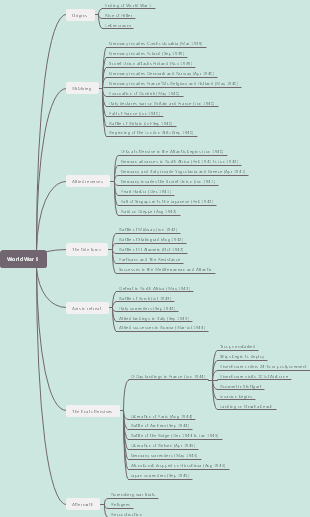
Embark on an educational journey through one of history's most significant events, the French Revolution. Our article provides a detailed analysis of the social, economic, and political factors that led to this period of upheaval. From the storming of the Bastille to the Reign of Terror and the rise and fall of Robespierre, discover the key phases that shaped the course of French and global history. We explore the Revolution's enduring legacy, including its influence on modern democratic principles and the eventual establishment of a republic. This rich narrative is essential for history buffs, academics, and students alike.
Edited at 2021-04-18 07:31:50Recent works
View more works>>
- Recommended to you
- Outline